- Home
- MCQs
- Cases
- Flashcards
- Your Feedback
- Become a reviewer
- More student books
- Student Apps
- Join an e-mail list

A 31-year-old married Vietnamese woman presented to the Accident and Emergency department following an episode of haemoptysis in which she had expectorated 250 mL fresh red blood. Nasopharyngeal examination by the ENT surgeons was normal, and a chest radiograph (Fig. 47) in the Accident and Emergency department was unhelpful, although bronchial wall thickening was noted behind the heart (arrow). There was no further bleeding, and she was discharged with an outpatient appointment. Over the next few days, she continued to expectorate small clots of blood mixed with discoloured phlegm.
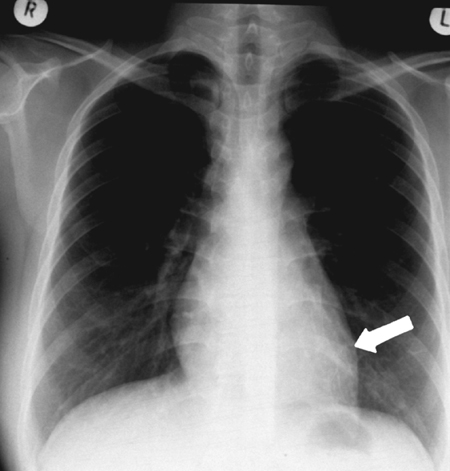
Figure 47 Chest radiograph
At her outpatient appointment, she reported a 10-year history of recurrent, intermittent haemoptysis in which she had expectorated small quantities of fresh red blood, sometimes mixed with bronchial secretions. She had been investigated by several doctors, but chest radiographs were normal, and she had been reassured that the bleeding was from the upper respiratory tract. For the 6 months before her presentation to the Accident and Emergency department, she had coughed up small quantities of blood every 2–3 weeks (<50 mL), but there was no associated fever, wheeze or breathlessness on these occasions. Two weeks before presentation to the Accident and Emergency department, she developed a cough productive of purulent sputum and night-time sweating. As a child, she had suffered with whooping cough, but there was no other past medical history of serious chest illness or tuberculosis. She is a non-smoker.Examination was normal. She did not have finger clubbing, anaemia, cyanosis or lymphadenopathy. Chest examination was unremarkable. The breath sounds were vesicular, and there were no crackles or wheezes. Routine blood tests, including an erythrocyte sedimentation rate (ESR) and C-reactive protein and sputum microbiology including examination for tuberculosis, were normal. The grade 1 Heaf test was consistent with immunity to tuberculosis.
1. What are the most common causes of haemoptysis, and from which circulation does bleeding occur?
2. Is haemoptysis life-threatening, and how is the severity of bleeding classified?
3. What are the clinical features that may help establish the diagnosis? What is the most likely cause in this case?
4. What investigations would you perform to establish the diagnosis in this case?
Correct answer: Routine blood tests (white cell count raised in infection), including erythrocyte sedimentation rate (ESR) (raised in vasculitis) and C-reactive protein (raised in infection). Specialist blood tests (D-dimers for pulmonary emboli, Aspergillus precipitans, vasculitis screen) may be required. Sputum microbiology may isolate infective organisms (pneumonia, abscess, Aspergillus) or acid-fast bacilli (tuberculosis). A screening Heaf test may detect tuberculosis. Chest radiography should be obtained in all patients. It may provide important diagnostic information including evidence of a mass, cavity or abscess. CT scans with contrast may detect the site of bleeding, tumours, vascular malformations and other structural abnormalities. In this case, the CT scan demonstrated a grossly dilated bronchus (>10 mm) consistent with bronchiectasis in the anteromedial segment of the left lower lobe (Fig. 48a). Bronchoscopy is often required to detect endobronchial lesions and inhaled objects (e.g. tooth). Combinations of bronchoscopy and CT scanning have the highest diagnostic yield. Bronchial arteriography may be required to detect the site of bleeding (Fig. 48b).
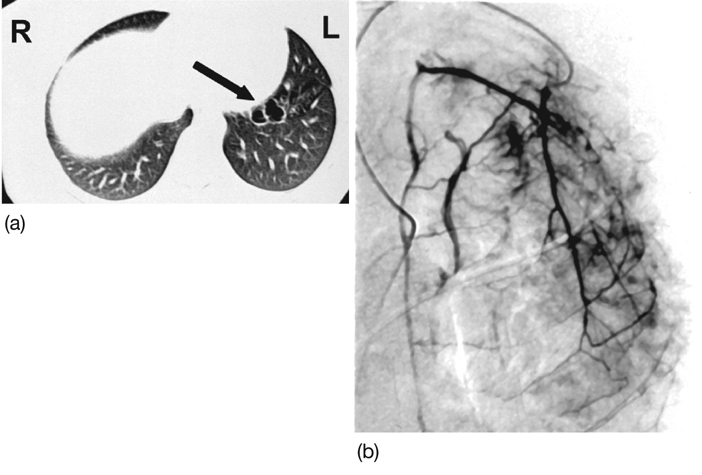
Figure 48 (a) CT scan and (b) bronchial arteriography.
5. What is bronchiectasis, and what causes it?
6. How should a large haemoptysis be managed?
Immediate control of haemoptysis is achieved at bronchoscopy by directing boluses of iced saline with epinephrine (10 mL; 1:10 000 dilution) at the bleeding site.
Bronchial angiography and embolization are the established therapeutic techniques for the initial control of haemoptysis. This procedure is initially successful in 70–100% of cases. The best results are described in patients with dilated bronchial arteries (e.g. bronchiectasis). Re-bleeding often occurs (~40%), and infarction of the anterior spinal artery with paraplegia is reported (~5%). Most studies agree that surgical therapy is associated with the best long-term outcomes for isolated lesions. Primary medical management may be mandatory because bleeding cannot be localized (widespread Aspergillus infection) or is not amenable to surgical resection of a pulmonary segment. In other patients, surgery will be contraindicated because of end-stage lung disease (FEV1 <40% predicted), poor cardiac reserve, unresectable cancer or severe bleeding diathesis.
Final diagnosis: Bronchiectasis of the anteromedial segment of the left lower lobe.