- Home
- MCQs
- Case Studies
- Your Feedback
- Become a reviewer
- More student books
- Student Apps
- Join an e-mail list

A 70-year-old man presents with a 12-hour history of not being able to pass urine. He has had problems in the past with his ‘waterworks’ and has noticed that his stream is very slow and barely reaches the pan of the toilet. He has no significant co-morbidities. On examination he has a palpable bladder and his genitals are entirely normal. Examination of his prostate reveals a 60-g benign-feeling prostate. You diagnose him with acute urinary retention.
1. What catheter would you use and why?
Two days later he returns to the hospital to have a trial without catheter. Unfortunately, he is unable to pass urine and develops supra-pubic discomfort and a palpable bladder. He needs a catheter while he awaits a definitive procedure in 6 weeks’ time.
2. Using the same principles as before, describe what catheter you would use?
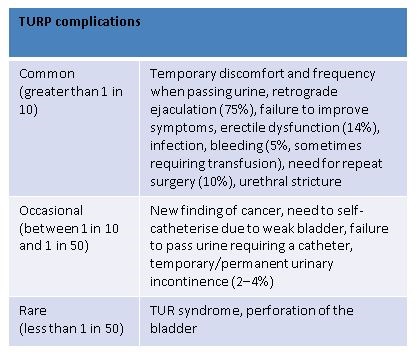
3. What definitive procedure is he going to have and what are the risks?
Correct answer:
Transurethral resection of the prostate (TURP). The risks can be split into common, occasional and rare.
4. What is TUR syndrome?
5. What factors were found to have an influence on the risk of developing TUR syndrome?