A 55-year-old man is referred for investigation of an enlarged spleen. He attended his GP because of discomfort in the left upper abdomen, and his GP found him to have a palpably enlarged spleen. He is otherwise well and asymptomatic. The GP performed a full blood count, which showed the following results:
Hb 111 g/L
WBC 3.2 × 109/L
White cell differential – normal
Platelets 95 × 109/L.
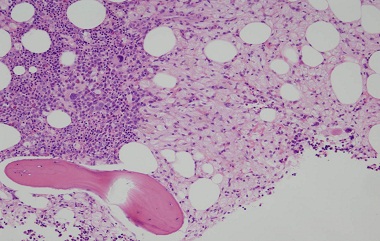
Blood film – as illustrated.
-
(a) What is the differential diagnosis?
Show Answer
Correct answer: He is anaemic and has reduced levels of white cells and platelets – this is pancytopenia which could result from pooling of blood cells within the spleen and accelerated destruction of blood cells from all three lineages. Causes of splenomegaly are listed in Box 19.2. Chapter 19
-
(b) What special features in the history will you enquire about?
Show Answer
Correct answer: A detailed history should be taken, relating to clinical features relevant to the wide range of causes of splenomegaly. These include liver disease (alcohol, travel, drugs, past illnesses including hepatitis, a history of jaundice, pruritus or bone pain suggesting osteomalacia); lymphoma (symptoms of bone marrow failure, systemic ‘B’ symptoms of lymphoma including weight loss, night sweats, fever or pruritus); tiredness and shortness of breath indicating cardiac disease. His family history and ethnic origin could be relevant as he may have a haemoglobinopathy or a storage disease. A travel history and enquiry about fever and night sweats is also relevant as infections can cause splenomegaly. Infections that can cause splenic enlargement include bacterial endocarditis, some viral infections, e.g. infectious mononucleosis, hepatitis viruses, brucellosis, histoplasmosis and malaria.
-
(c) What further tests will you undertake?
Show Answer
Correct answer: A wide range of tests is indicated in the light of the wide ranging differential diagnosis, and the precise nature of the tests will be determined by the detailed history.
Liver function tests, coagulation and other assessment of liver disease including titres for hepatitis viruses and tests for chronic liver disease, e.g. caeruloplasmin, alpha-fetoprotein, serum ferritin to exclude haemochromatosis.
Tests to exclude haematologic malignancy. A careful examination of the blood film is important, e.g. to exclude hairy cell leukaemia; occasionally lymphoma cells may be seen in peripheral blood and a peripheral blood differential must be carefully performed. Flow cytometry of peripheral blood cells can sometimes reveal a minor population of lymphoma cells.
A CT scan or other imaging of the abdomen should be undertaken to carefully assess spleen size, liver size and texture and look for other intra-abdominal pathology, e.g. lymphadenopathy. A bone marrow aspirate and trephine biopsy should be undertaken to look for infiltrative conditions. A liver biopsy may also be appropriate. A monospot can be done to look for infectious mononucleosis, other tests for infections should be undertaken depending on the clinical circumstances, e.g. peripheral blood screening for presence of malaria parasites.
See Chapter 5 for further details.
In the case discussed here, the man was of Ashkenazi Jewish descent. His serum β-glucocerebrosidase activity was reduced, the serum chitotriosidase activity (a marker of macrophage activity) was grossly elevated, and bone marrow showed confirmatory features of Gaucher disease.
-
(d) What are the complications of splenomegaly?
Show Answer
Correct answer: Splenomegaly can cause upper abdominal discomfort. A markedly enlarged or tender spleen could undergo spontaneous rupture. An enlarged spleen is usually functionally deficient and hyposplenism may be present – with an increased susceptibility to infection, and the presence of typical changes in the blood film (target cells, Howell–Jolly bodies in red cells). Hypersplenism refers to the presence of pancytopenia with reduced lifespan of blood cells from all three lineages. Splenomegaly is also associated with increased blood flow in the splanchnic circulation and this can cause portal hypertension.
-
(e) Would you advise splenectomy?
Show Answer
Correct answer: No. The cause of splenomegaly should first be established. Complications of splenectomy are discussed in Chapter 19.