-
(a) What are the differential diagnoses?
Show Answer
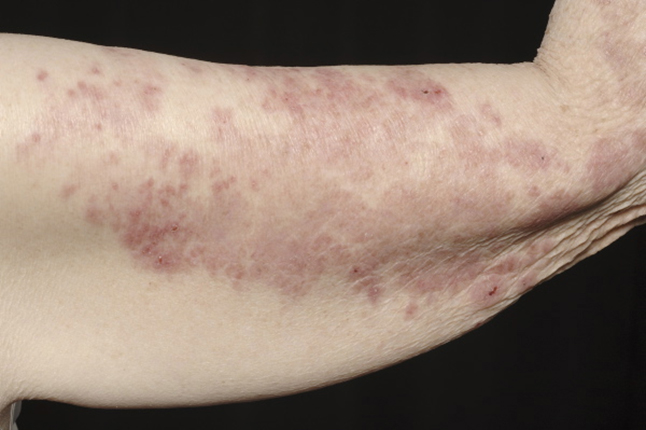
This presentation has a wide differential diagnosis. Psoriasis, drug allergy, eczema and contact dermatitis may all present with this clinical picture. All except psoriasis are likely to be itchy. The history can help and detailed past history, family history and drug history need to be taken. Particular points to clarify are history of atopy, any problems with skin contact with new or old products, and any new oral drugs commenced. A specific history of photosensitivity was given, leading to worsening of the non-itchy scaly rash.
-
(b) What investigations are needed?
Show Answer
Patch testing may be needed to exclude allergic contact dermatitis. Blood tests needed include blood count, urea and electrolytes, liver function, autoantibody screen with ANA (anti-nuclear), anti-double stranded DNA, anti-Ro (anti-SSA) and anti-LA (anti-SSB) antibodies to exclude subacute and systemic lupus erythematosus. Skin biopsy is needed for histology and immunofluorescence.
-
(c) What is the most likely diagnosis?
Show Answer
The most likely diagnosis is discoid lupus erythematosus (DLE). This is the most common form with localised or widespread scaly red papules and plaques with central atrophy and scarring. DLE is more common in women, with peak incidence in the forties. Photosensitivity is present in 50%.
-
(d) Can this lead to other conditions?
Show Answer
Approximately 1–5% of DLE cases progress to SLE. SLE is a multi-system disease affecting women (8 : 1 ratio) aged 30–40 years. A butterfly rash can occur (in 50% of patients) on malar areas of the cheeks. There is no atrophy and alopecia occurs in 20% of cases. Other manifestations include fever, arthritis, vasculitis, Raynaud’s phenomenon, oral mucosal ulceration and nail fold capillary changes.
-
(e) How do you treat this condition?
Show Answer
Treatment options include oral, intralesional and topical corticosteroids (potent to very potent), anti-malarials (e.g. hydroxychloroquine) and dapsone. Sunscreens are essential, with strict sun avoidance.